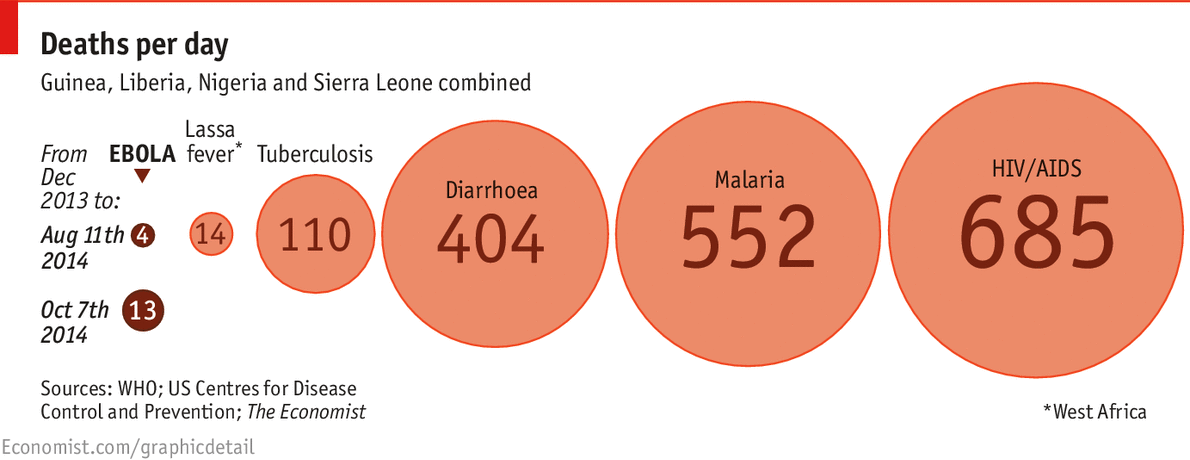
Ebola still barely rates among the continent’s big killers. Far
more deaths are attributable every day in west Africa to malaria,
diarrhoea and HIV/AIDS. But the spread of infections means that death
rates are rising fast: from four a day in August to 13 now. There are no
licensed treatments or vaccines (although scientists are working all
out to rectify that). The assumption that an Ebola outbreak could always
be managed—the disease is hard to catch and people are only contagious
when they are showing symptoms—is under strain.
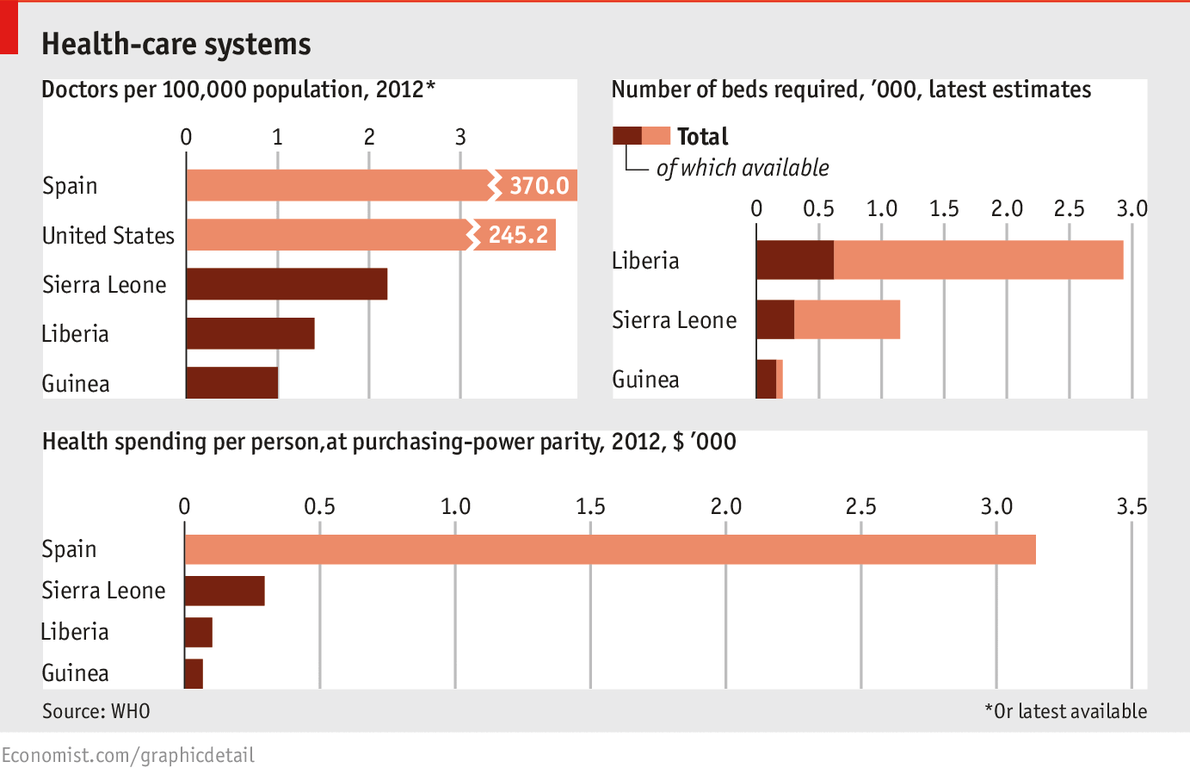
The inadequacies of the health-care systems in the three
most-affected countries help to explain how the Ebola outbreak got this
far. Spain, whose first locally transmitted case was confirmed on
October 6th, spends over $3,000 per person at purchasing-power parity on
health care; for Sierra Leone, the figure is just under $300. The World
Health Organisation estimates that Liberia needs just under 3,000
treatment beds for Ebola; its current capacity is 620. The United
States, which suffered its first Ebola fatality this week, has 245
doctors per 100,000 people; Guinea has one. The particular vulnerability
of health-care workers to Ebola is therefore doubly tragic: as of
October 5th there had been 390 cases among medical staff in the three
west African countries, and 227 deaths.
Ebola is not just a medical emergency, but an economic one.
Sick people cannot work; fear of sickness keeps others from coming to
work. Transportation and travel is disrupted. An impact assessment by
the World Bank, released on October 8th, estimated the short-term impact
of the outbreak on the economies of Guinea, Liberia and Sierra Leone in
terms of forgone GDP at $359m. Depending on whether the outbreak is
contained quickly or slowly, the damage will continue into next year;
under the Bank’s gloomier “High Ebola” scenario, the economic loss to
Liberia in 2015 would be the equivalent of 12% of GDP.
>>Ebola still barely rates
among the continent’s big killers. Far more deaths are attributable
every day in west Africa to malaria, diarrhoea and HIV/AIDS.
I don't think your method of calculating deaths per day from Dec 2013
onwards is a fair comparison. For endemic diseases such as malaria,
there will be very little difference between the average long term value
and the instantaneous value. For ebola, where deaths are doubling every
few weeks, there is of course a very large difference.
We can estimate the instantaneous ebola deaths per day from the figures for Oct 1 and Oct 8 provided by WHO:
deaths per day = (4033-3439)/7 = 85
This is very different from your long term average of 13 per day.
Furthermore, ebola is already a significantly bigger killer than malaria
in Liberia:
Liberia ebola deaths = 2136
Liberia malaria deaths = 40 deaths per 100k people = 1600 (2010 WHO data)
Although well researched, this article is typical of many in that it
fails to capture the real concern about Ebola -- the rapid doubling up
of cases and deaths.
See
https://sites.google.com/site/ebolagraph/


I don't think your method of calculating deaths per day from Dec 2013 onwards is a fair comparison. For endemic diseases such as malaria, there will be very little difference between the average long term value and the instantaneous value. For ebola, where deaths are doubling every few weeks, there is of course a very large difference.
We can estimate the instantaneous ebola deaths per day from the figures for Oct 1 and Oct 8 provided by WHO:
deaths per day = (4033-3439)/7 = 85
This is very different from your long term average of 13 per day. Furthermore, ebola is already a significantly bigger killer than malaria in Liberia:
Liberia ebola deaths = 2136
Liberia malaria deaths = 40 deaths per 100k people = 1600 (2010 WHO data)
Although well researched, this article is typical of many in that it fails to capture the real concern about Ebola -- the rapid doubling up of cases and deaths.
See https://sites.google.com/site/ebolagraph/